How I've largely overcome low back pain

Back pain. Lots of folks have it, at least in The West. Chairs, shoes, inflammatory diet (and the associated obesity all contribute to this problem. You can get cranky about that last point but it’s just the physics of how a bigger than ideal belly affects the low back. And knees. And…
All kinds of things factor into low back pain. Something like 80% of folks in the US will experience low back pain at some point. Nearly 30% of the US population will suffer some form of chronic back pain, which is defined as lasting longer than 3 months.
I suffered from terrible intermittent low back pain for nearly 20 years. This is likely some kind of Karmic payback for my approach to helping folks with low back pain when I was a physical therapy assistant. I really liked working with people but the way some folks carried on about their back pain left me scratching my head. I’ve had multiple broken bones, including compound fractures. I’ve actually broken a cervical vertebrae (did not know it at the time…only found it via later X-ray) and although all that stuff certainly hurt, I did NOT conduct myself the way folks do when their back is out.
Sweating, barely able to stand, move or breathe.
I thought many of our patients were malingerers. Some might have been, but my lack of empathy was due to one simple fact: I’d never YET experienced a day of back pain in my short life. Well that certainly did change, and I’ll get to that story momentarily, but it might be worth looking at a little pathophysiology of back pain and then loop back into what I did to bugger mine, and what I’ve done to get back to some semblance of functionality.
Low Back Pain 101
I’m going to end up referencing a lot of people I’ve worked with, all of whom are better at the anatomy of the back and how alterations therein can cause pain, but this is how I’ve organized this material to make sense for myself. I see the vast majority of back pain being some kind of SI joint (sacroiliac) dysfunction or disk issues.
The SI joint is the interface between the sacrum and the hip bones. All manner of nerves come out of the spine at this area (in particular the sciatic nerve). It’s in close proximity to the strongest, most used muscles of the body. There are lots of performance and mobility needs.

Grok was kind enough to spin up this image. Which is kinda close, but also freakishly wrong!! Anyway, these structures must transmit force from lower to upper body (and vice versa). It has nerves, muscles, vessels…lots of stuff going on. Because of the interface between the spine and the more mobile iliac bones, we hope that things are functioning properly, in particular we hope that those two iliac bones are symmetrical with each other and playing nice with the sacrum, nerves etc. The iliac bones can get out of alignment by one side being higher than the other and, to a lesser degree, one side being forward of the other. This situation in and of itself does not guarantee back pain, but it does set the stage. Think about if you are squatting or deadlifting fairly heavy and one hip is higher than the other. Think about activities like walking, running or rucking if one leg is “shorter” than the other (often a result of the hip being higher on one side.
I had this condition in spades. I’ve dug through old photos trying to find an example but my right hip was remarkably higher than my left hip for a looong time. This was largely the result of a number of years of Thai boxing which puts a lot of emphasis on the rear leg for kicking. I did traditional stretching a lot (could drop down into the front and middle splits cold, I can still hit the front splits cold at 53 YO…which this flavor of mobility ironically hid my deeper problems). I was visibly crooked, but I did not have the tools to fix that issue. Like I said, that specifically was not enough to drop me into back-pain hell, I had to start doing CrossFit for that!
Some of you might recall I co-founded the first and fourth CrossFit affiliate gyms. There were lots of good things that came of my time with CrossFit, and I guess a catastrophic back injury can be included in that if I have a rosy enough perspective to acknowledge it as a learning opportunity. I was down in Santa Cruz training with Greg Glassman and the HQ crew when I was introduced to a (then) brand new movement, the glute-ham sit up:

If you are not familiar with the movement, it is a remarkably long range of movement and introduces a massive eccentric load to the abdominals. I forget what the precise structure of the workout was…I think it was part of a chipper or longer, multi station circuit, but I do remember my first exposure to this movement, at my “Coach’s” prodding, was 75 repetitions.
It absolutely ruined me. This was a bit before the awareness of rhabdomyolysis, but the day after this workout my abs were visibly swollen and distended. I think I was not far off of Diastastis Recti.
Well, since one must be prepared for “The Unknown and Unknowable” we were to pull max dead lifts two days after my Prison Shower Scene with the glute-ham-situp.
It didn't go well.
DL’s require a profoundly rigid trunk and when your abs are inflamed and shredded as if they were a bucket of Southern Cole-Slaw…bad things happen. I had 465 lbs just past the knees when my abbs just catastrophically failed. This was a heavy but doable weight for me, but one moment I was reaching the end of the lift and the next I was folded in half like a question mark. I nearly lost continence (seriously, I had to struggle to not pee and shite myself simultaneously) I crawled out of the gym “Lt. Dan” style, I could barely make it to my car. My lower abdominal wall was profoundly distended and I could not remotely get into a full, extended and upright position. I was in unbelievable pain for the better part of two weeks. A sneeze could just about render me unconscious from the combo of sharp pain and burning afteraffects. Sleep was hell as there were no comfortable positions. I had radiating pain down both the front and back of both legs (although mainly my right side) and I was starting to experience some weird muscle atrophy in places that were apparently not receiving proper nerve innervation.
In addition to having some likely SI joint issues from my previous Thai boxing, I’d given myself a high amplitude, high load disk injury. My symptoms were consistent with a disk rupture in which disk fluid interacts with various nerves and can cause truly horrific pain and infirmity.
This was the summer of 2004 and my main way of supporting myself was running a gym! Demonstrating movements. Correcting form…walking around all day. This was a rough time that would extend on for the better part of 20 years. As tough as this was, it was actually better for me than content creation and book writing, which is what my career shifted into by ~2007 forward. Gym life presented challenges, but kept me moving. Sitting on my ass (or standing at a desk) for hours each week was far worse for me back.
I found some nominal ways to cope. Chiropractic with Active Release Technique could get me out of a flare but it was short lived and did not address my underlying issues. Sitting, standing, any type of spinal loading (squatting, deadlifting…bag of groceries!) could lay me out for a week or two at a shot. I looked at everything I could find on back pain and, for ME, none of it was particularly helpful. The name-brand folks in the back pain game had advice like “don’t do the things that make your back hurt!” Which in some ways is spot on (For example, sitting crosslegged in the floor did and still does present huge problems for me) but it also became kinda ridiculous: rounding my back (spinal flexion) could hurt things, as could sitting without low back support, standing in one place, walking slowly (short strides). Too soft of a bed was a problem (I tend to sleep on my left side, which appears to exacerbate my hip imbalance…sleeping on the floor is great for my back, terrible for everything else!!) What ultimately happened is the variety and intensity of movement I did was dramatically curtailed. Little volitional spinal flexion, when I sat I crossed my legs and had awesome back support. This kinda put things into a holding pattern but I’d still get injured about once every 6-8 weeks with about one week spent lying on the floor bemoaning my life.
The Fix
So, I HAVE found a route to minimal back issues (last 2 years have been quite good) but it’s been a process. I’m going to mention several folks that have helped me. I'm likely not going to do justice to what each provided, but they have all for sure been important. The first person that gave me a rubric to really address my back pain was Dr. Carolyn Dolan. Dr. Dolan is a DPT and an expert in the Mckenzie method of back pain management. The Mckenzie method is simple yet powerful: The thought is that a bulging disk can contact the spinal cord or nerves and cause pain. By putting the spine into graded flexion, extension, and lateral movement (side glide), one can mechanically suck the disk back into the proper place, reduce back muscle spasms, address pelvis imbalance, and reduce pain.

This was remarkably helpful as it can begin to address both of the primary back pain causes: disk and SI joint. One can move through both flexion and extension, which CAN be the cause of a back pain flare, but complete avoidance of those positions is just about impossible and does not (again) address root cause. Alternating between 1A and 1B can be both therapeutic and diagnostic. If one has problems getting into extension for example (certainly an issue I have struggled with) the side glide (1E) can reset the pelvis so one CAN get into extension. A slick thing Dr. Dolan showed me was if I’m jammed up and can’t get into extension standing, I can lie prone and then off-set my hips to the right or left. For me, because my right hip tends to elevate, I’d lie on my stomach, then scoot my hips to the left a bit,then press up into cobra position. I’d first find an easy spot that would work, do 5-10 reps, lie flat, inch my hips to the right, repeat, and just keep doing that until I could do a prone back extension, then work back to standing and see if I can get into extension with the moderate load of standing.
I know this probably reads like an Ikea instruction manual, but a qualified practitioner (or likely even some Youtube investigating) can put a lot of context to this.
This was the first concrete strategy I found that I could reel myself back from being totally incapacitated. I think a lot of what was happening here is actually taking the low back into a graded flexion/extension. Again, even though those positions CAN trigger an event, not training them shrinks the capacity you have. This SHOULD have been some insight for me of where to go, but it took some other smart folks to help button up more pieces of this puzzle.
Sarah and Grayson Strange
The next folks who really helped on this process are my good friends Sarah and Grayson Strange of Basis NY. I’ve known these two for a long time and they are some of the most knowledgeable and accomplished coaches I’ve ever met. They were early to the FRC/Kinstretch scene and are just phenomenal. Although the Mckenzie method material helped me get out of injury/spasm situations, I was still getting injured and the problems seemed to be migrating to my hips. Sarah and Grayson did a remote assessment looking at my mobility and strength in some positions I’d never really thought about. Again, I could drop into the front splits easily, could get close to the side splits…I was mobile, right? Not really. In addition to being super weak in both my spinal flexion and extension (due to not loading those movements, more on that later) I had terrible hip mobility, specifically internal and external mobility. This “90/90” hip position illustrates both capacities:

The front leg is challenging external rotation of the hip. The back leg is challenging internal rotation. I was shite on both, but particularly internal rotation. Something folks in the FRC world are savvy to is a lack of internal rotation is all but a guarantee of an eventual hip replacement as the hip joint does not do what it needs to do as far as movement. This shifts an undue burden onto not just the hip/sacrum interface, but when your damn hips are tight, movement that SHOULD happen at the hips ends up being shifted to your back!
Let me say that again, as you cannot over-appreciate the significance, and if there is literally only one thing you take from all this, this might be the most important:
If you lack proper HIP mobility (including things like internal/external rotation) when you do movements, the load will get shifted to your back because your hips are not functioning properly. An, you will most likely get injured. Again, and again.
If you recall, I said I had some weird achy issues with my hips. An x-ray showed some early degenerative hip issues on my left side, which the symptoms have completely resolved with this work.
As great as the Mckenzie method is, it did not address these other issues. I did remote coaching with Sarah and Grayson for the better part of two years and although I still have a lot of work to do, the FRC/Kinstretch methods of not just mobilizing these movement patterns, but strengthening them, made a huge impact on me. I apologize for not going into detail here but the FRC/kinstretch methodology is complex, at least at first. They train the end range of joint mobility the same way most people train squats and deadlifts…which I think is why it works so well. Have you ever done a max-effort internal rotation of the hips? I never had, and not only did it show (in terrible strength and mobility) but I was totally unprepared for how demanding this work is. Sarah and Grayson do excellent remote coaching,I cannot recommend them enough, but you might look around and see if you have an FRC practitioner near you.
Knee-Over Toes+Low Back Ability
The final two influences to my back rehab journey include the “Knee over toes guy” (Ben Patrick) and “Low Back Ability” (Brendan Backstrom). I forget precisely how both of these gentlemen got on my radar but I think a Youtube video popped up of Ben talking about his “Knee over toes lunge” and how it favorably impacted not just his knee health, but his back pain.
Everything I Know About The Lower Back
That’s a really solid exploration of Ben’s take on back issues, and it was interesting as I’d seen some of Ben’s work, thought it was cool, but fortunately, I’ve never really had knee issues. Ben has a storied history of knee issues, lots of surgeries, partial patella replacement and he was in rough shape. He loves basketball but had a hell of a time doing it and ironically, could never dunk.
Until he developed this approach to all things performance (Ben Studied under one of my favorite strength coaches, Charles Poliquin). Ben is known for his knee stuff, but in one of his videos he described how the KOT lunge really helped his back issues. This is what that looks like:

HOLLY shite but that knee is over the toe! AS important and impressive as that is, the rear leg is where the back maintenance story is. You see, that leg is being both stretched and strengthened, right at the hip flexor and psoas. Muscles that if either weak, tight, or both (which sitting produces in spades) ends up tugging on the pelvis in a way that fosters back pain. ALSO: That deep lunge position seems to be magic for addressing pelvic imbalances. When I started working my way through the progressions for this movement, my back made a major leap forward. If memory serves, I’ve only had one significant “back outage” since incorporating this into my program and since also incorporating movements like Jefferson curls, specific flavors of back extensions and side bends, (knock on wood) my back has not gone out.
Before I move on, I just want to mention, there is a regression/point of entry for just about ANYONE on this (and all of these) movements. This is a look at how Ben has progressed his 70 YO mom through the system:
My Mom’s Experience With Knees Over Toes
You may start with a chair and no weight. Then, slowly, you build capacity and start lowering your front leg, eventually adding weight. I’d look at this a LOT like I do back issues: if you never let your knees go over your toes in training, you will have a capacity gap when you do it in real life. You will never jump, run, land, without your knees going over your toes. You will, at some point, lift something, bend, sneeze etc in a way that puts your back into dynamic flexion or extension. You can sneak up on training the capacity of these ranges OR you can neglect them and have it potentially bite you later.
As I started looking into all this I also found Brendan (low back ability) and although both Ben and Brendon (also Grason and Sarah now that I think of it) use a LOT of the same movements (KOT lunge, romanian DL, back extensions,Jefferson curls etc) this is how it all rolled out to me and started making both sense and an impact.
Brendan had a sprinting background and found himself in an awful pain, spasm, pain cycle with his back. Standard PT did not really hit the root cause, he’d “baby” his back and then, picking up a piece of paper or a sneeze would leave him on the floor in serious pain. Brandon recommended a battery of movements, including the KOT lunge but also some specific takes on the back extension, side bend and Romanian deadlift. This is well detailed in the below video:
The REAL Reason You Have Back Pain (we were lied to)
I know this is a lot to take in, and it’s really just scratching the surface, but holy smokes, all of this has transformed my life. I’ll give some direct insight into what I do on a weekly basis, but I want to reiterate a point regarding some commonalities with all of this, from FRC to Ben to Brandon:
-ALL of these movements are necessary
-ALL of these movements are scaleable
-They should all be performed at a level that is pain free
-Then progressed from there
My current training
So, how do I incorporate all of this into my week? Here is a template I put together that's informed by what I’ve learned from Sarah/Grayson, Ben and brandon:
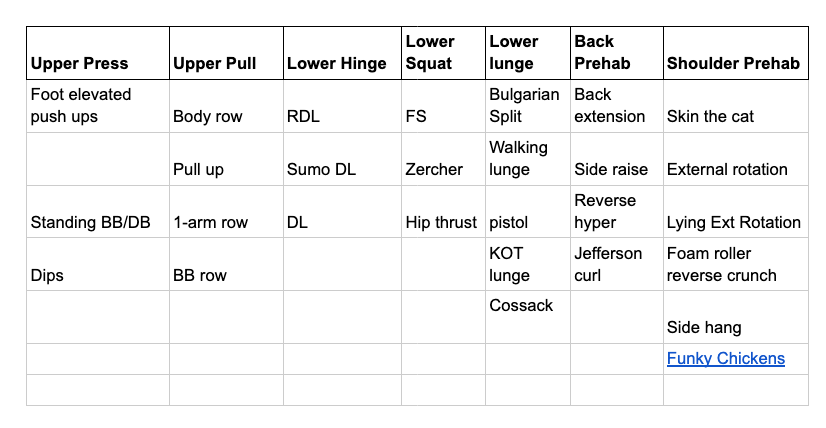
What the heck is a Funky Chicken? Glad you asked!
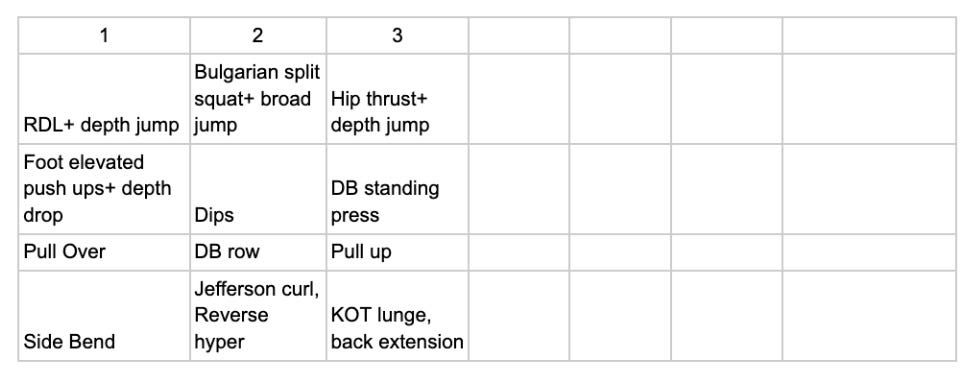
So, the upper material are the movements I pull from, the lower is the three day split I use. Each day has some kind of a press, a pull, a lower body movement, then trunk and rehab movements thrown in. I’ve shifted to doing dips and foot elevated pushups (using a weight vest where appropriate) as I get a greater range of movement on these vs benching, and it feels great on my shoulders.
For some of the movements I’ve added “complex training” in that I will do a strength focussed movement like RDL’s, then follow that about 30 seconds after the set with either a depth jump or some kind of bounding plyometric. As we age the thing we lose the fastest is power production and I hope this will stave that off. I like the push ups for this as I’ll do my heavy-ish set, take off the weight vest, then go from my push up handles and hop to the floor…about a 12” drop! I really feel these and I do think it’s helped put some pop back in my movements.
The RDL is the only DL I’m really doing, and I will occasionally put in some kind of front squat, but axial loading, directly loading the spine, can still give me problems. I think the mechanics of the RDL are such that I don’t get huge axial loading from that and can go fairly heavy. I can go hard on split squats and have no issues with my back.
Recent Update: I have not played with the Zercher Squat much previously, but have done it the past 3 weeks and really like it. I have a tough time with back squats as the direct axial loading irritates my lumbar disk injury. Front squats are better, but they too eventually reach a point of loading that irritates the disk. The Zercher squat may pull so much of the load forward, making me carry the load through braced abs, that it really minimizes axial loading. All I know for certain is I’ve been able to load this movement more than the other squat variants and with nothing but benefits.
Progression consists of a “Bulgarian” inspired approach. I work up to a heavy-ish 5-6 reps, then back things down about 20% and get in a few more sets for volume. I tinkered with much higher rep schemes, in the 20-30 rep range and it just cratered my recovery. This all feels great overlaid with some conditioning and 2-3 days per week of jiujitsu.
FRC/Kinstretch integration
In broad brush strokes I do targeted FRC movements before training as part of a general warm-up (be that lifting, jits or conditioning). I’ll also do some work between sets. Let’s say its split squats and dips. I’ll work hip, shoulder and lat mobility between those sets.
Most evenings I watch a show with one of my girls and will work my way through the couch stretch, interna/external hip mobility via the 90/90 position and usually a bit of foam rolling and shoulder work. This tends to be more relaxed, passive stretching work in these positions (held for 3-5 minutes) and I think the consistency is key to keeping my back happy.
Meds and Closing Thoughts
Quick disclaimer: I’m not a doctor, this is not medical advice. But holy smokes do I have a lot of experience in this realm! Just mentioning all this so you can best understand my thinking and progress.
I’ve not had to use ANY type of pain medication for over two years for my back. This is amazing as there was a long period of time where this was a regular occurrence. I think we all know things like NSAIDS can be bad news over the long haul. They absolutely are. BUT, what I found is that if I tweaked something, 600-800mg of ibuprofen immediately would often get me out of trouble in a few days. Without it, things might drag on a week. That seems like a clear and easy decision then, right? Well, NSAIDS can worsen chronic back pain. I’ve been aware of this tradeoff for quite some time and it led me to sometimes take ibuprofen when my back was in a serious state, and sometimes I did not. I’m fairly certain taking the ibuprofen shortened any given event. The literature suggests it may have set me up for subsequent issues…I’m not totally sure it did as the research on this stuff tends to look at folks who use these products almost constantly.
Just a quick diversion along that line: I generally feel pretty good. I think I’m holding together fairly well for 53 years of activities like youth football, Thai boxing, jiujitsu etc. THAT SAID, any given day I’ll have a little shoulder issue, some low grade back crankiness (mornings I’m still a little uncomfortable most days until I get moving) etc. I forget how I got onto a given research track but I found some articles suggesting some non-trivial performance enhancing effects of acetaminophen (tylenol), particularly for endurance activities. I know that stuff is hell on one's liver but I tried taking a nominal dose with some NAC and glutathione precursors to try and mitigate the downsides and…WOW!! I felt great. Turns out not having 8-10 little niggling pain points is amazing for feeling good! ALSO: low-moderate dose tylenol likely exhibits anti-depressant effects…which also tends to have synergy with reducing pain. Why am I mentioning all of this? If I just took a bit of tylenol and or ibuprofen on the regular, I’d likely feel GREAT. (Until I felt way less than great). I get why folks end up taking this shit by the handfuls, and we are not even talking about stuff like opiates or valium. It sucks being in pain and uncomfortable, these magic little pills work (short term) miracles in how we feel, but likely come at a high cost later. I mention all this to just create some space for you to think about all of this. Pain meds (even over the counter) likely offer benefit in targeted situations. If you can’t sleep due to pain, you won't heal! But that said, I’d be incredibly wary of habituating to these substances. Do everything you can on diet, phototherapy, mobility to get as much juice out of your natural healing ability as you can. Then, IF you really need some pain relief, use it in a targeted and acute fashion.
I think that’s it for now! There is a lot here but it’s also just the very surface of these modalities. If you suffer from low back pain I can’t encourage you enough to explore all of these modalities. When I was in pain I swear it felt like my batter was used up at 5x the speed when I’m not hurting. At points it made me question how long I wanted to live. My back issues were easily in the “severe” category and I’ve been able to regain a remarkable amount of capacity and by extension, really improve the quality not just of my life, but the lives of the folks around me. Not surprisingly, we do not show up at our best as dads, husbands, friends etc. when we are in crippling pain. Check this stuff out, ask questions and please, don’t give up!
Properly performing the “McGill Big 3” saved me from my L5/S1 herniation discomfort and pain. I’m in maintenance mode now but it took me 2 years to figure it out.
My lumbar spime MRI scan looks like a pretzel, yet I manage to stumble along pretty well for an old fart. We are spending the summer at our second home in Greece. Back home, I swim for 90 minutes, five days a week, and I plan to continue doing so here in Greece. I don't take any pain meds, and I seem to be getting along pretty well.